Bacterial toxins in dead teeth: The health risk – and our solutions
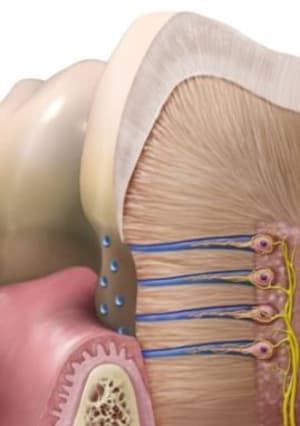
Although a tooth may appear as hard, lifeless tissue, it is a living organ. The hard outer enamel protects soft tissues, blood vessels and nerve tissue inside the tooth. Between the enamel and the nerve lies a layer of dentin tissue, which is literally interwoven with microscopic tubes, or dentin ducts. Their total length in a tooth is about 3 km (ill. 1)
Healthy (living) teeth have their own nutritional and self-cleaning mechanism of dentin ducts, using dentinal fluid. Under normal physiological conditions, it flows from the nerve through the dentin to the enamel and from there into the oral cavity.
In numerous studies, Dr. Ralph Steinman and Dr. John Leonora have shown why this mechanism plays a key role in tooth health:
• Dentin does not have a vascular supply. The flow of dentinal fluid outwards from the tooth transports nutrients from the blood vessels of the dental marrow (pulp) to the dentin and keeps it healthy
• The direction of the dentinic fluid flow prevents acids and bacteria from entering the tooth from the mouth cavity
• The alkaline pH of dentinal fluid helps neutralize acids produced by microbes on the surface of the tooth.

But what about dead teeth with purified dentin ducts? These teeth are de facto hollow and therefore lack the abovementioned vascular supply. They are therefore deprived of their natural cleaning mechanism. Even the most precise treatment of dentin ducts under the microscope cannot eliminate all bacteria in the complex system of root canals ‒ it is simply not possible to flush kilometers of dentin ducts. Another problem is that the size of bacteria is 0.6‒1 micrometers (μm), which can easily penetrate into dentin ducts with a diameter of 1‒3 micrometers. (ill.2 Bacteria at the entrance to the dentine ducts in a dead tooth.)
Due to the ease of passage of bacteria into the microscopic structures of dentin ducts, the complete disinfection of the entire (dead) tooth is impossible.
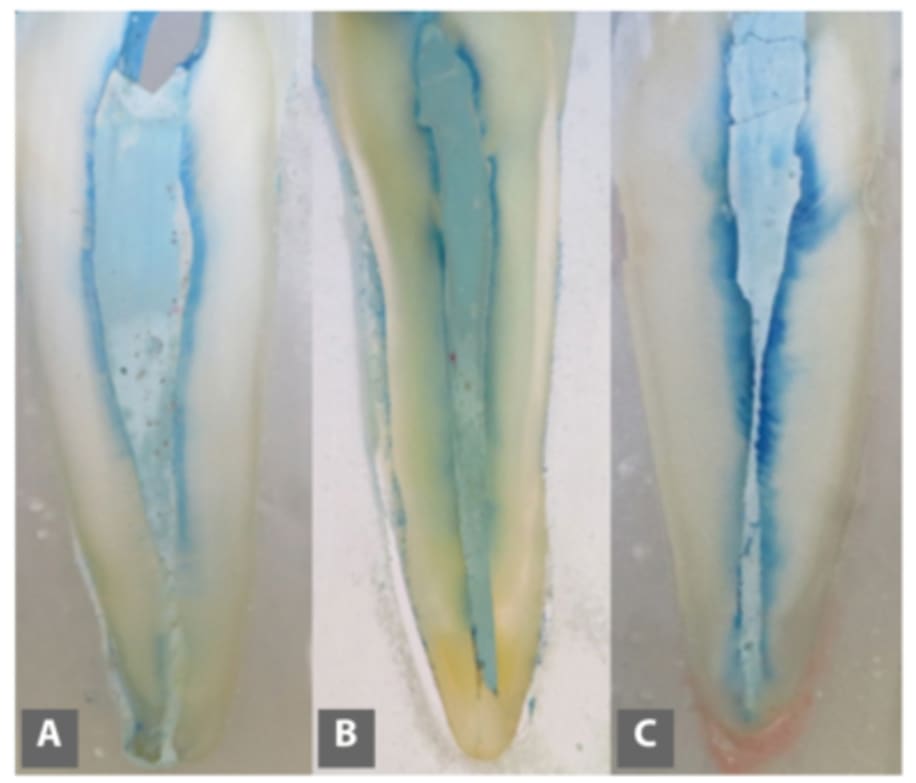

Studies confirm that after mechanical cleaning of the root system, an entire 35‒40% of the channel surface remains untreated. (ill.3 Comparison of the anatomical structure of the dental pulp (red) and the limited possibilities of mechanical treatment of the canal surface (green)) Subsequent rinsing with sodium hypochlorite (Savo) removes larger residues of infected soft tissues in the central canal only, and as shown in Fig. 4 (see blue colouring), the flush is only effective in approximately 10% of the length of the dentine tubules. (Fig. 4: Example of the rinsing solution penetration depth in dentine tubules. A – passive rinsing; B – rinsing with sonic activation of the solution; C – rinsing with ultrasonic activation of the solution.)
And that’s the problem. The mechanically treated tooth remains forever infected with various types of anaerobic bacteria that thrive on tissue residues, and their metabolism produces toxic waste substances (e.g. thioether or mercaptan). When chewing, these bacteria and their toxins enter the lymphatic system of surrounding tissues and from there enter the bloodstream and spread into the entire body.
The solution is the surgical removal of these teeth, including the inflammatory tissue under them. It is very important to thoroughly remove the periodontal ligament, disinfect the alveolus with ozone and, if necessary, use the patient’s own blood plasma for faster healing. Vitamins D3, K2 and A support successful healing too, and also act effectively in the prevention of jaw bone necrosis.